 |
 |
 |
Vol.
21, No. 3
June 2016
The North Carolina Child Treatment Program
Helping Child Welfare Professionals Find the Right Mental Health Treatment for Every Child
Child welfare professionals spend a lot of time trying to navigate the mental health system on behalf of families. Most of us have heard the phrase "evidence-based treatment models," or EBTs. We realize there are mental health treatments out there that could make significant improvements in children's lives, but there are challenges in accessing EBTs: how do you know which treatments are likely to help a particular child? And how do you find the right kind of provider when you need one?
The North Carolina Child Treatment Program (NC CTP) is a tool that can help you connect with EBT providers in your county. Founded in 2006, the NC CTP is focused on dissemination of evidence-based mental health treatments for infants, children, and adolescents coping with attachment difficulties, psychological trauma, traumatic bereavement, and behavioral challenges. This focus makes NC CTP a useful partner for county DSS agencies. And conversely, DSS child welfare social workers are critical to NC CTP realizing its mission.
Fidelity Matters
When looking for a specific evidence-based treatment model, it's important to find a clinician who provides the model with fidelity, meaning as the model was designed and tested.
For example, one of the most well-studied and effective interventions for children who have experienced trauma is Trauma-Focused Cognitive Behavioral Therapy (TF-CBT). There have been at least 12 randomized controlled trials that have shown better outcomes for children and youth who receive TF-CBT compared to other types of treatment or to no treatment (NCTSN, 2012). To have the best chance of improved outcomes, you want to be sure the clinician is providing TF-CBT with fidelity--that is, in the same way it was provided in those studies.
To ensure clinicians provide EBTs with full fidelity, NC CTP provides learning collaboratives that last from one to two years, depending on the model. Clinicians participate in multiple day-long trainings and also receive intensive case consultation. Those who successfully complete a collaborative are included on a roster that can be searched by county at http://ncchildtreatmentprogram.org/
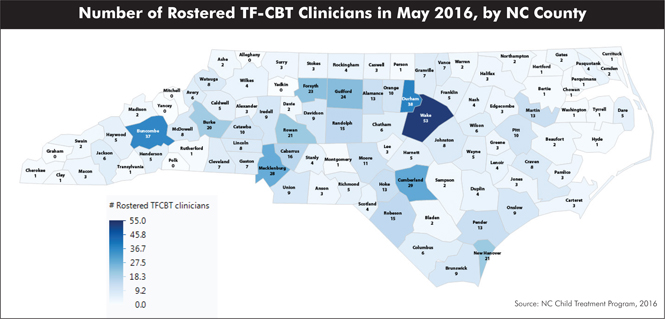
TF-CBT in North Carolina
TF-CBT learning collaboratives have been taking place since 2006. There are currently 373 rostered TF-CBT clinicians practicing across the state. Each month new clinicians complete the learning collaborative requirements and become rostered, so be sure to check the site regularly. The map below shows the number of rostered TF-CBT clinicians in each county as of May 2016.
Children age 3-21 who have experienced traumatic grief or other forms of trauma may benefit from TF-CBT. This therapeutic model helps clients develop the skills to tolerate their trauma memories and manage their symptoms. It also helps clients change how they view themselves, their history, and the world, allowing them to reduce symptoms, heal, and build resilience.
What about Younger Kids?
To participate in TF-CBT, children and teens need to be able to remember and verbally describe their experiences. A common challenge for the child welfare system is that the largest category of children served is those from birth to age 5 (Duncan, et al., 2016). Many of these children are too young or don't yet have the verbal or cognitive skills needed for TF-CBT.
In the past, many people believed infants and young children were too young to be affected by traumatic experiences or exposure to chronic stress. However, we now know young children experience the effects of trauma well before they are able to describe what's happening to them. And of even greater concern, we know that early childhood trauma has a significant impact on children's ability to securely attach to their primary caregivers, which in turn can significantly affect their emotional and cognitive development (NCSTN, 2010).
One of the most exciting developments in North Carolina's mental health system is the spread of an evidence-based treatment model specifically for children from birth to age 5. Child-Parent Psychotherapy (CPP) was developed by psychologists Alicia Lieberman and Patricia Van Horn. The treatment is designed for infants and children who have experienced trauma or significant stress, or whose parents have significant stress or histories of trauma. In other words, it is a model with the potential to meet the needs of many families served by the child welfare system.
CPP recognizes that the parent-child relationship is the most important factor in a young child's life, as well as the greatest source of long-term healing and support. As a result, CPP focuses on the parent-child dyad, seeking to create a secure attachment and a caregiver who can remain attuned to and be protective of the child even in the face of adversity. Studies of CPP show that it has been successful in reducing symptoms in both parents and children, and in strengthening attachment (see below).
A new CPP learning collaborative will begin in fall 2016. This means clinicians may be able to accept referrals from county DSS agencies before the end of 2016. Keep your eyes on the NC CTP website (www.ncchildtreatmentprogram.org) for more information.
Child welfare and mental health professionals often find each other's systems challenging to understand and navigate. Working together, DSS and NC CTP can serve as a bridge, helping to find the right treatment and the right provider for each child.
NC Child Treatment Program Models: The Basics |
Trauma-Focused Cognitive Behavioral Therapy (TF-CBT)
Child-Parent Psychotherapy (CPP)
Sources: Lieberman, Van Horn, & Ghosh Ippen, 2005; Lieberman, Ghosh Ippen, & Van Horn, 2006; Ghosh Ippen, Harris, Van Horn, & Lieberman, 2011 |