 |
 |
 |
Vol.
21, No. 3
June 2016
Partnering for Excellence
Working to Improve Services and Outcomes for Children and Families Affected by Trauma
As this issue shows, a lot of energy is being put into trying to improve outcomes for children and families involved with the child welfare system in North Carolina, especially those who have experienced trauma. Partnering for Excellence (PFE), a Duke Endowment-funded effort in Rowan County, is another great example.
History and Goals
Partnering for Excellence began in 2012 when The Duke Endowment provided funding to Benchmarks, an alliance of nationally-accredited human service agencies in North Carolina, to redesign the way the child welfare and mental health systems interact to:
- Provide trauma-informed services to support improved child and family outcomes;
- Reduce costs by helping both systems avoid unnecessary use of high-end services; and
- Reduce the need for future CPS involvement in families currently receiving child welfare services.
The pilot of PFE got off the ground in July 2013 in Rowan County, where the department of social services (DSS); Cardinal Innovations, the county's mental health managed care organization (MCO); and private mental health providers have been collaborating to increase their focus on trauma and the use of evidence-based practices. The Center for Child and Family Policy at Duke University is evaluating the PFE pilot.
The Model
PFE is a different way of doing business for agencies serving child welfare-involved children ages 5-17 and their families. Key elements of the PFE approach include the following.
Initial Trauma Screens. In Rowan County, DSS workers screen all children entering CPS in-home and permanency planning services for trauma exposure. Capitalizing on the good work being done elsewhere in the state, they do this using the trauma screening tool developed by Project Broadcast. This is a one-page questionnaire completed by the DSS child welfare worker after talking with the child, birth parents, foster parents, and any other relevant sources of information about the child.
To date, 90% of young people screened by Rowan DSS as part of PFE have experienced some kind of trauma. Among children in DSS custody, every single one (100%) has screened positive for trauma (Benchmarks, 2016).
Trauma-Intensive Comprehensive Clinical Assessments (TiCCAs). After screening, DSS refers all children with trauma histories for a TiCCA. These in-depth evaluations are done by specially trained private mental health providers. The goal of a TiCCA is to fully understand what the child has experienced and how those experiences have affected and are continuing to affect the child and family.
To conduct a TiCCA, a provider must be trained to deliver Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) and have an additional day of training in case conceptualization. PFE clinicians include in the TiCCA holistic recommendations that discuss not only the child's needs for mental health treatment but also school, parenting, pro-social behaviors, and anything else that may be needed.
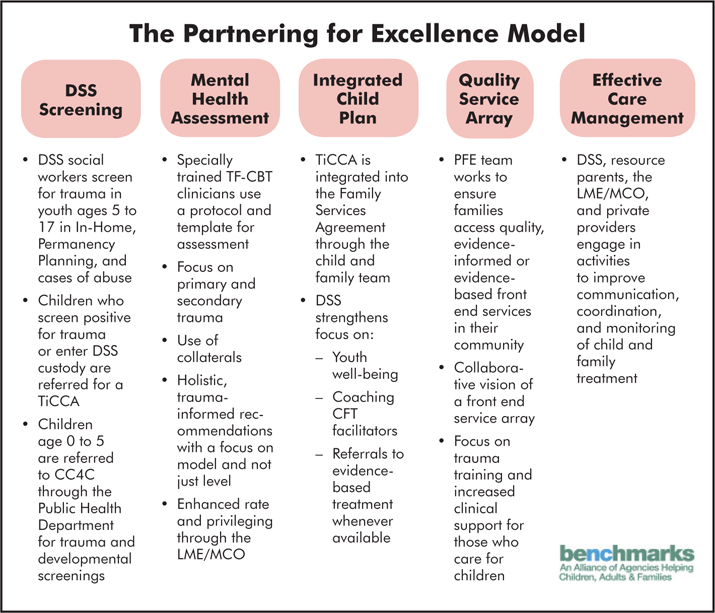
Integrated Child Plan. The TiCCA helps DSS and its partners start out on the same page. DSS can incorporate information from this assessment into the family services agreement. Just as importantly, it uses this information to make referrals to (and advocate for) the right services and an appropriate model of care for each child. Guided by TiCCA results, the MCO can authorize needed services right from the start. Appropriate services help children heal from trauma and learn coping skills, which have the potential to help them stay in their own homes, stabilize placements, or expedite permanency.
Quality Service Array. PFE has Rowan DSS, Cardinal, and mental health providers talking about what else the community needs to serve families better. In addition to expanding the number of local TF-CBT providers, since PFE began Rowan has added new parenting courses. The idea is to create a community that is trauma-informed, trauma-aware, and trauma-responsive.
Effective Care Management. A very important dimension of PFE is the model's emphasis on the need for those serving DSS-involved families to work together to improve communication, coordination, and monitoring of child and family treatment. This requires a lot from all parties, including building a strong foundation by attending training together, more formal agreements (such as memorandums of understanding), and committing to participation in ongoing collaborative meetings.
Many of those involved have concluded the added effort is worth it because it helps the mental health and child welfare systems understand each other and their interdependence. As one stakeholder put it, "From a systematic view, you can't do child welfare without mental health partnering" (Benchmarks, 2016).
PFE Outcomes
It's too early in the evaluation of the PFE pilot to talk about the extent to which this effort can help communities achieve the project's long-term goals of improving child and family outcomes, avoiding unnecessary high-end services, and reducing repeat child maltreatment. That said, preliminary evaluation results comparing children before and after PFE came to Rowan County seem promising.
For example, as Figure 1 shows, since the start of PFE there has been a decrease in the percentage of young people diagnosed with ADHD and conduct disorder, while the number diagnosed with PTSD has increased. One explanation for this change is that because providers now have more information about trauma histories, they see children's symptoms and behaviors in a new light.
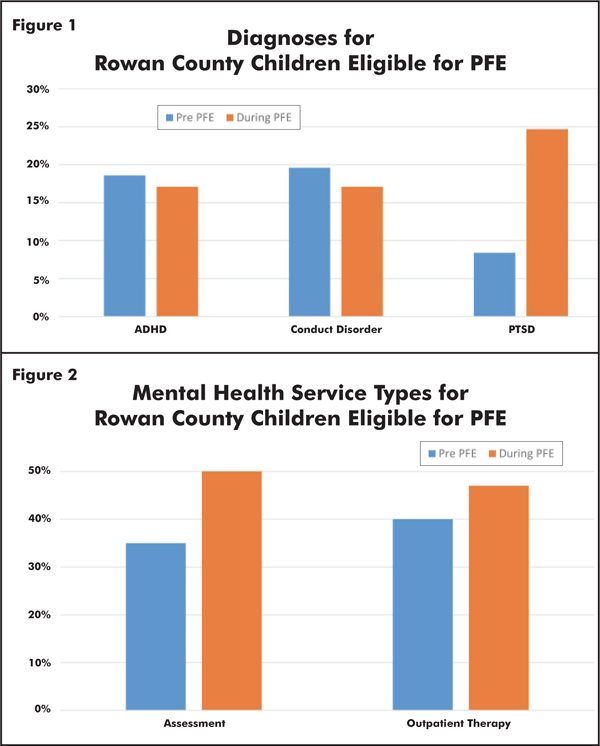
PFE also seems to be having an effect on the mental health services DSS-involved children receive. As Figure 2 shows, since PFE, more children are being assessed and, perhaps because TiCCAs are so thorough, more are receiving outpatient therapies such as TF-CBT.
What's Next
Evaluators will continue to collect information to better understand whether PFE ultimately has the desired impact. In the meantime, Benchmarks and its partners, with the continued support of The Duke Endowment, are beginning to work with additional counties. Cleveland County Department of Social Services and its MCO, Partners Behavioral Healthcare, started implementing the PFE model earlier this year, and the project will likely add at least one more county in the next year.
To Learn More about PFE
For more information, contact Tara Fields at tfields@benchmarksnc.org.